Lab testing in telemedicine is defined as the integration of diagnostic specimen analysis into virtual care workflows, enabling clinicians to make evidence-based decisions without requiring patients to visit a physical clinic. This integration transforms telemedicine from a consultation-only service into a full diagnostic platform. Platforms like Renewmd demonstrate how the role of lab testing in telemedicine extends beyond convenience, providing the objective clinical data that drives accurate diagnosis, medication titration, and long-term patient monitoring. Technologies such as FHIR-based order systems, point-of-care testing devices, and at-home collection kits have made this integration both practical and clinically reliable.

How lab testing integrates with telemedicine workflows
Effective telemedicine and diagnostic testing depend on a structured order pathway that moves from virtual consultation to specimen collection to result delivery without losing clinical integrity. The industry standard for this is the FHIR ServiceRequest resource, a hierarchical data structure that captures the ordered test, specimen type, collection date, and handling instructions in a single digital record. This level of detail matters because a lab result is only as reliable as the metadata attached to it. A creatinine value without a documented collection time, for example, is difficult to interpret in the context of hydration status or medication timing.
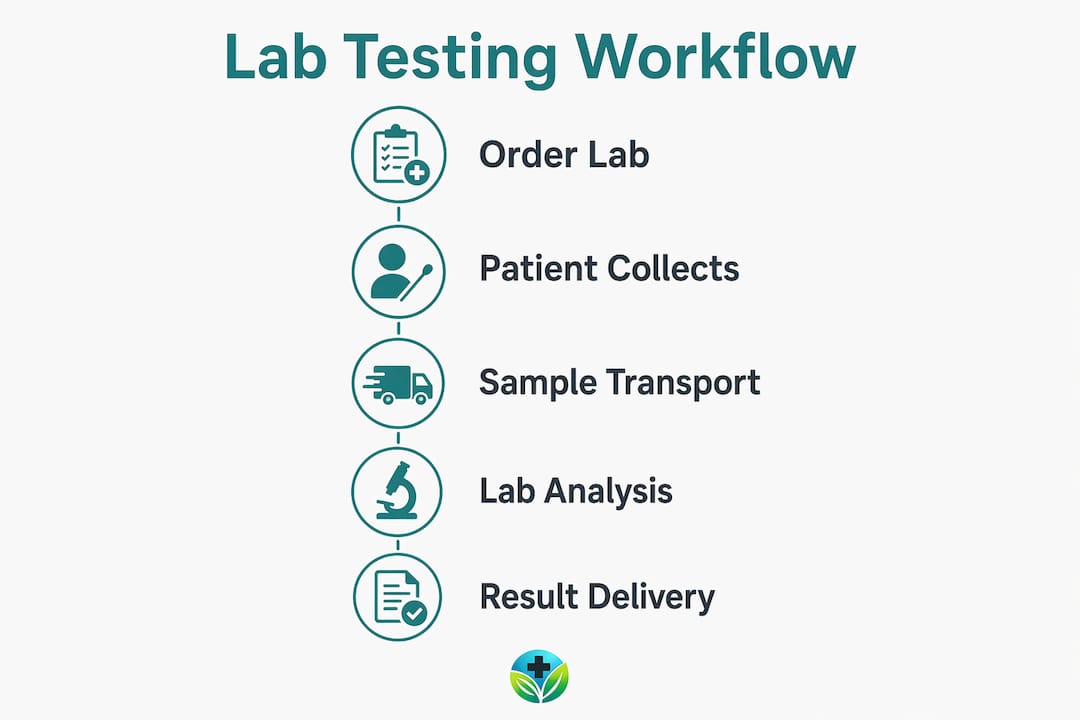
The workflow typically follows four steps:
- Virtual consultation and order generation. The clinician conducts a video or asynchronous visit, identifies the diagnostic need, and generates a digital requisition through an integrated platform.
- Patient-directed specimen collection. The patient visits a local draw site such as Quest Diagnostics or LabCorp, or uses an at-home collection kit for capillary blood, urine, or saliva samples.
- Specimen transport and laboratory analysis. The sample is processed at a certified reference laboratory, with results transmitted electronically back to the ordering provider.
- Result integration and clinical action. Results populate directly into the electronic health record, triggering provider review and, when necessary, a follow-up virtual visit or medication adjustment.
The weakest link in this chain is step two. Patient follow-through on lab orders placed during virtual visits is measurably lower than after in-person encounters. Standardizing specimen metadata exchange using FHIR reduces errors and improves auditability across multi-site telemedicine workflows, but it does not solve the human adherence problem. That requires a separate strategy, addressed in the challenges section below.
Pro Tip: If you are a clinician ordering labs through a telemedicine platform, confirm that your system captures specimen collection date and method at the time of order, not just at result receipt. Missing pre-analytical metadata is one of the most common sources of interpretive error in remote testing workflows.
What lab testing technology for telehealth looks like today
The most significant shift in lab testing technology for telehealth is the movement away from centralized laboratory dependence toward decentralized, near-patient testing. Two categories define this shift: point-of-care testing (POCT) and at-home collection kits.
| Feature | Point-of-Care Testing (POCT) | At-Home Collection Kits |
|---|---|---|
| Setting | Clinic, pharmacy, or urgent care site | Patient's home |
| Sample type | Whole blood, urine, nasal swab | Capillary blood, urine, saliva |
| Turnaround time | Minutes to 1 hour | 24 to 72 hours |
| Accuracy | High, validated devices | Variable, depends on handling |
| Best use case | Acute decisions, rapid triage | Chronic disease monitoring, screening |
| EHR integration | Direct, real-time | Delayed, requires upload |
POCT bypasses transport delays and delivers results fast enough to support same-visit clinical decisions. A clinician managing a patient's anticoagulation therapy remotely, for instance, can use a POCT INR device at a local pharmacy partner to adjust warfarin dosing within the same telehealth encounter. This eliminates the 24 to 48-hour lag that traditionally separates testing from treatment.
At-home capillary blood collection kits, such as those offered by companies like Everlywell or LetsGetChecked, extend access further. However, sample stability is time and temperature sensitive. A pilot study analyzing approximately 7,600 proteins found significant proteomic changes when samples were delayed beyond 48 hours or stored above 4°C. This means that a patient who collects a sample on Monday morning but fails to ship it until Wednesday has potentially compromised the clinical value of that test. Logistics management in at-home testing is a clinical safety factor, not just an operational convenience.
Consumer health wearables from companies like Apple, Garmin, and Fitbit add a third layer of data. These devices provide physiologic metrics such as heart rate variability, sleep patterns, and activity levels. Wearables correlate moderately with clinical metrics, but the FDA does not regulate most wellness device claims. Best practice is to cross-validate wearable data with certified laboratory results rather than treating device outputs as diagnostic conclusions.
Pro Tip: When using at-home collection kits, instruct patients to refrigerate samples immediately after collection and ship on the same day using the prepaid overnight courier included in the kit. A 48-hour window is the outer limit for most analytes.
What are the main challenges in telemedicine lab testing?
The benefits of remote lab testing are real, but so are the barriers. Understanding these barriers is the first step toward building workflows that actually close diagnostic gaps.
- Lower ordering and completion rates. A cohort study found 14.3% fewer high-value tests ordered during virtual visits compared to in-person encounters, with 13.1% fewer tests completed. This gap is not trivial. High-value tests include metabolic panels, lipid profiles, and kidney function markers that directly inform chronic disease management.
- Pre-analytical variability. Shipping delays beyond 48 hours and inadequate refrigeration materially alter analyte results. When a patient mishandles a sample, the error is invisible to the clinician reviewing the result. The number looks real, but it may not reflect the patient's actual physiology.
- Administrative friction. Digital requisition systems vary in quality. Some telemedicine platforms generate lab orders that arrive at draw sites without proper specimen instructions, causing rejection or recollection.
- Patient education gaps. Many patients do not understand why a lab order matters or what happens if they skip it. Without context, a lab requisition feels like optional paperwork rather than a clinical necessity.
"Over 80% of at-risk patients miss necessary follow-up lab tests, with analysis of 84,259 records showing only 15% received recommended albumin-to-creatinine ratio testing, projecting a 43% kidney disease risk among those who were missed." Follow-up testing gaps represent one of the most preventable sources of disease progression in remote care.
The solution is not simply ordering more tests. Systematic alerts triggered by incomplete lab orders are shown to be necessary to prompt patient action, because ordering alone does not guarantee completion in remote settings. Platforms that track the full lifecycle of a lab order, from generation through patient completion to result receipt, close this gap more effectively than those that treat the order as the endpoint. Patient education on proper sample collection and follow-through is equally critical, particularly for patients managing chronic conditions remotely.
How lab results shape clinical decisions in telemedicine
Objective lab data reduces diagnostic error in ways that symptom reporting alone cannot. A patient describing fatigue during a virtual visit could have a thyroid disorder, anemia, vitamin D deficiency, or poorly controlled diabetes. Without a metabolic panel and complete blood count, the clinician is working with incomplete information. With those results, the differential narrows immediately and treatment becomes precise.
Consider diabetes management as a concrete example. Monitoring hemoglobin A1c, fasting glucose, and kidney function tests such as eGFR and the albumin-to-creatinine ratio gives a telemedicine provider a complete picture of glycemic control and end-organ impact. This is the same data set used in an endocrinology office, delivered remotely. The clinical decision quality does not have to differ from in-person care when the diagnostic data is equivalent.
POCT integration into electronic health records supports pharmacist dosing decisions and nurse monitoring interventions by providing timely data to the full care team. This is interprofessional collaboration enabled by data access, not geography. A pharmacist reviewing a patient's INR result in real time can flag a dosing concern to the prescribing clinician before the patient leaves the virtual encounter.
Patient trust also improves when lab data is part of the care experience. Receiving a result, having it explained during a follow-up virtual visit, and seeing a treatment adjustment based on that result reinforces that remote care is medically substantive. For patients managing weight with GLP-1 receptor agonists like Semaglutide or Tirzepatide, baseline and follow-up labs including liver function, lipid panels, and kidney markers are not optional monitoring. They are the clinical foundation that makes dose adjustments safe and evidence-based.
Key takeaways
Lab testing is the diagnostic backbone of telemedicine, and without it, virtual care remains a consultation service rather than a complete clinical encounter.
| Point | Details |
|---|---|
| FHIR standards improve accuracy | Structured lab orders using FHIR ServiceRequest capture specimen metadata that prevents interpretive errors in remote workflows. |
| Sample handling is a clinical safety issue | At-home samples must be refrigerated and shipped within 48 hours to preserve analyte integrity and result reliability. |
| Completion gaps require active intervention | Telemedicine visits see 14.3% fewer high-value tests ordered and 13.1% fewer completed, requiring alert systems to close the gap. |
| POCT accelerates clinical decisions | Point-of-care testing delivers results within minutes, enabling same-visit treatment adjustments without centralized lab delays. |
| Lab data enables personalized treatment | Integrated results such as A1c, eGFR, and lipid panels allow clinicians to titrate medications safely and monitor outcomes over time. |
Why integrated lab testing is the line between good telemedicine and great telemedicine
I have reviewed enough telemedicine programs to recognize a pattern: the ones that produce strong patient outcomes treat lab testing as a core clinical function, not an afterthought. The ones that struggle treat it as optional, something patients will get around to eventually.
The frictions are real. Patients forget. Samples get delayed. Orders fall through the cracks in platforms that were not built to track the full lab lifecycle. I have seen patients on GLP-1 therapy go months without kidney function monitoring because no one built a follow-up alert into the workflow. That is not a technology problem. It is a clinical design problem.
What I find genuinely encouraging is how much the technology has matured. FHIR-based ordering, at-home collection kits with overnight logistics, and POCT devices that feed directly into EHRs have removed most of the structural barriers. The remaining gap is clinical culture. Providers and platforms need to treat telehealth lab adherence with the same rigor they apply to medication adherence. A prescription without monitoring is incomplete care, whether it is delivered in an office or through a screen.
The future of telemedicine's diagnostic capability depends on platforms that close the loop automatically, not ones that rely on patients to self-navigate a fragmented system. That is the standard worth building toward.
— Raymond
How Renewmd integrates lab testing into weight care
Renewmd builds lab testing directly into its GLP-1 weight management programs, treating diagnostic monitoring as a clinical requirement rather than an add-on. Every treatment plan includes provider consultations, medication delivery, and lab-supported monitoring through licensed U.S. clinicians, so patients on Semaglutide or Tirzepatide receive the metabolic and kidney function data their care requires. There are no hidden fees and no separate billing for the diagnostic components of care. If you are exploring medically supervised weight management through telemedicine, the RenewMD weight care guide explains exactly how the clinical and diagnostic process works from enrollment through ongoing monitoring.
FAQ
What is the role of lab testing in telemedicine?
Lab testing in telemedicine provides the objective clinical data that clinicians need to diagnose conditions, monitor chronic diseases, and adjust treatments remotely. Without lab results, virtual care is limited to symptom-based assessment, which reduces diagnostic precision.
Why are fewer labs completed during virtual visits?
Research shows 14.3% fewer high-value tests are ordered and 13.1% fewer are completed during virtual visits compared to in-person encounters. The primary causes are reduced patient follow-through and the absence of automated alert systems to prompt completion.
How accurate are at-home lab collection kits?
At-home kits are accurate when samples are processed within 48 hours and stored below 4°C. Delays beyond 48 hours and inadequate refrigeration cause significant proteomic changes that compromise result reliability.
What is point-of-care testing and how does it support telehealth?
Point-of-care testing (POCT) delivers diagnostic results at or near the patient care site within minutes, eliminating the delays associated with centralized laboratory processing. POCT supports telemedicine by enabling same-visit clinical decisions, particularly for anticoagulation management, infection diagnosis, and metabolic monitoring.
Which lab tests matter most for GLP-1 telemedicine programs?
Baseline and follow-up labs for GLP-1 therapy typically include a metabolic panel, lipid profile, hemoglobin A1c, eGFR, and the albumin-to-creatinine ratio. These markers monitor glycemic control, kidney function, and cardiovascular risk, providing the clinical data needed to adjust dosing safely over time.