The role of medication delivery in telehealth extends well beyond logistics. For healthcare professionals and policymakers, it sits at the intersection of regulatory compliance, clinical workflow design, and patient outcomes. Yet most discussions treat delivery as a side note to the consultation itself, which is a significant error in framing. Getting medication into a patient's hands through a telehealth model requires navigating DEA rules, state pharmacy laws, Risk Evaluation and Mitigation Strategy (REMS) program mandates, and remote monitoring protocols. This article addresses all of it with the specificity that operational decision-making demands.
Table of Contents
- Key Takeaways
- The role of medication delivery in telehealth frameworks
- Regulatory frameworks governing telehealth prescribing
- Remote patient monitoring and medication management
- Operational challenges and best practices
- Future trends and policy considerations
- My perspective on getting medication delivery right
- How Renewmd integrates medication delivery in weight care
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Delivery is a clinical function | Medication delivery in telehealth directly affects adherence, titration, and patient outcomes, not just convenience. |
| Regulatory complexity is layered | Federal rules like the Ryan Haight Act and state-level variances create distinct compliance obligations for each program. |
| RPM closes the care gap | Remote patient monitoring transforms passive delivery into active medication management with measurable clinical benefits. |
| Operational resilience is required | Programs must build fallback dispensing options and certification verification to survive rapid regulatory shifts. |
| Policy should follow evidence | Aligning telehealth medication policy with clinical outcome data protects access for rural and underserved populations. |
The role of medication delivery in telehealth frameworks
Telehealth is often described in terms of video consultations or asynchronous messaging, but the care episode rarely ends there. For the vast majority of patients, the endpoint of a telehealth visit is a prescription, and what happens to that prescription defines whether the visit produced any clinical value at all.
Medication delivery models in telehealth fall into four broad categories: mail-order pharmacy fulfillment, direct shipment from a certified specialty pharmacy, local pharmacy pickup coordinated through electronic prescribing, and provider-dispensed supply in hybrid clinic-telehealth programs. Each model carries different regulatory requirements, patient communication needs, and adherence implications.
The impact of medication delivery on clinical outcomes is measurable. Rural patients, who represent approximately 20% of the U.S. population but are served by only 9% of physicians, face transportation barriers that make local pickup unreliable. Mail-order fulfillment integrated directly into the telehealth prescription workflow removes that barrier entirely. When delivery fails or is delayed, patients miss doses, adherence drops, and chronic conditions drift out of control.

The integration point matters too. When the prescribing platform connects directly to the dispensing pharmacy through electronic prescribing infrastructure, medication reaches the patient faster and with fewer handoff errors. Platforms that require patients to independently transfer prescriptions to a separate pharmacy introduce friction that disproportionately affects lower-health-literacy populations, the same groups telehealth was designed to serve.
Regulatory frameworks governing telehealth prescribing
Federal and state rules governing telehealth medication systems are not static, and recent developments have shifted the compliance landscape considerably.
The Ryan Haight Online Pharmacy Consumer Protection Act remains the foundational federal law. It restricts prescribing of Schedule II through V controlled substances via telehealth without a prior in-person evaluation. The DEA has maintained telehealth prescribing exceptions for DEA-registered practitioners meeting specific criteria, but those exceptions are narrowly defined. Programs that rely on remote prescribing for controlled medications need careful documentation workflows, not just a general understanding of what is permitted.
For non-controlled medications with elevated risk profiles, REMS programs introduce an additional compliance layer. The most high-profile recent case involves mifepristone, where SCOTUS maintained telehealth access and mail delivery while litigation continues. The ruling enforces REMS mandates, meaning pharmacies must complete certification agreements and use trackable shipping. Certified pharmacies must ship all covered medications with confirmed tracking, a requirement that has direct implications for program operations.
Key compliance steps for programs operating under these frameworks include:
- Verify DEA registration and prescriber eligibility before enabling telehealth prescribing of any controlled substance.
- Confirm pharmacy REMS certification status before routing prescriptions for high-risk medications.
- Establish documentation standards for any initial in-person qualifying visits required by federal or state law.
- Map state-level shield laws and variance policies, particularly for medications subject to political or legal dispute.
- Build patient communication protocols that explain delivery timelines and tracking requirements upfront.
Pro Tip: Policy compliance should be structured at the provider and workflow level, not just the platform level. Compliance gates built into the clinical intake process, prior to prescription generation, are far more defensible than after-the-fact audits.
State-level variances add meaningful complexity. Some states have enacted shield laws that protect providers prescribing certain medications via telehealth to out-of-state patients. Others have explicitly restricted telehealth prescribing in ways that conflict with federal guidance. For state-specific regulatory details, programs benefit from jurisdiction-by-jurisdiction review rather than relying on broad federal guidance alone.
Remote patient monitoring and medication management
There is a critical distinction that many telehealth program designers miss: delivering medication to a patient is not the same as managing that patient's medication. The role of technology in medication delivery extends into what happens after the package arrives.
Remote patient monitoring (RPM) is the clinical infrastructure that closes this gap. When patients use connected devices to measure blood pressure, blood glucose, or weight, that data feeds back to the care team in near real time. The care team can then act on deviations, adjust dosing, flag non-adherence, and communicate with the patient before a small problem becomes a hospitalization.
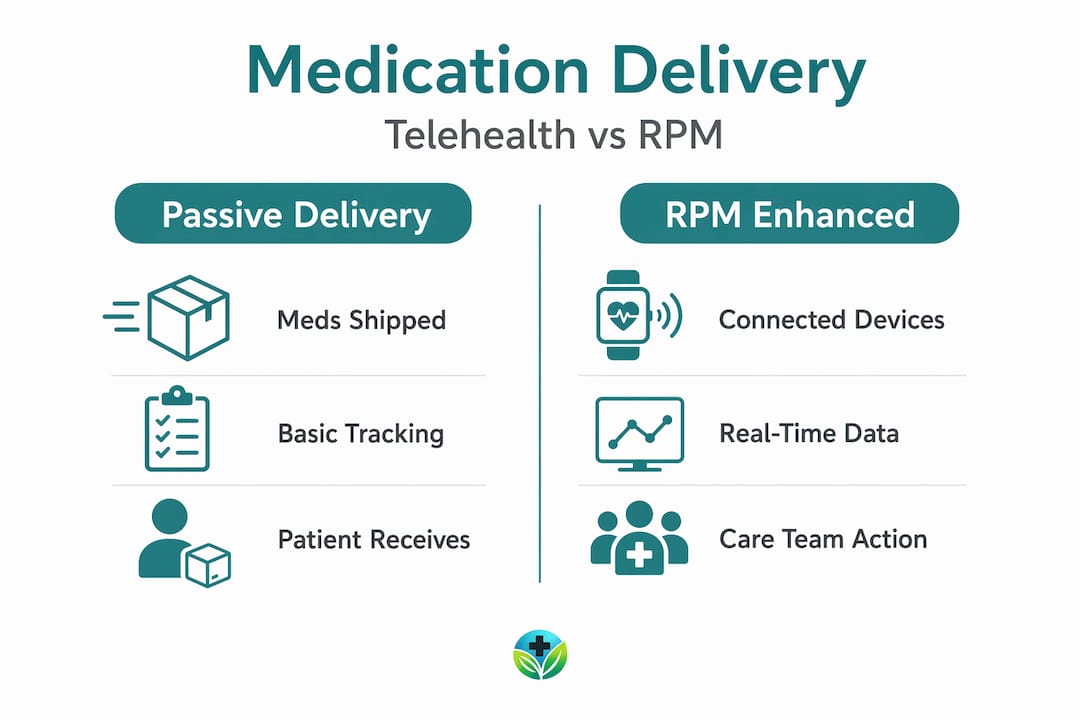
The following table illustrates how passive delivery and active medication management differ in practice:
| Dimension | Passive delivery only | Delivery plus RPM |
|---|---|---|
| Patient engagement | Receives medication | Receives medication and submits clinical data |
| Care team role | Prescribes and waits for follow-up | Monitors data, adjusts treatment proactively |
| Adherence tracking | Self-reported or absent | Device-confirmed with feedback loops |
| Outcome data | Delayed, visit-based | Continuous and actionable |
| Billing alignment | Prescription-based only | RPM billing codes available under CMS |
Research published in a peer-reviewed study shows that higher RPM engagement improves blood pressure control, and the benefit persists even when CMS adjusted reimbursement policy to allow billing with as few as two days of measurement per month. That policy shift, while reducing the administrative burden, did not reduce clinical value. Programs designed around patient-centered engagement rather than billing minimums saw the strongest outcomes.
Pro Tip: Separate your medication delivery logistics team from your clinical medication management team. When one group handles shipping, tracking, and pharmacy coordination, and another handles titration, adherence, and RPM data review, both functions improve. Conflating them creates accountability gaps.
Care team response time is the deciding variable. Rapid care team action on RPM data drives the clinical benefit. A monitoring program where data sits unreviewed for a week provides far less value than one where a pharmacist or nurse responds within 24 hours of a concerning reading.
Operational challenges and best practices
Building a telehealth medication delivery program that holds up under regulatory pressure, pharmacy supply variation, and patient communication demands requires deliberate design. The challenges are specific, and the solutions are equally specific.
The most common operational failure points include:
- Regulatory uncertainty: Rules governing telemedicine drug distribution shift faster than most compliance teams can track. Programs without a designated regulatory monitoring function find themselves out of compliance after policy updates they did not catch.
- Pharmacy certification gaps: Not all pharmacies that claim REMS certification are current. Routing a prescription to a pharmacy with lapsed certification can delay care and expose the program to liability.
- Patient communication breakdowns: When medications are shipped, patients need clear instructions on what to expect, including delivery timelines, storage requirements, and what to do if a shipment is delayed or damaged.
- Trackable shipping requirements: For REMS-covered medications, trackable shipping is not optional. Programs that use standard mail delivery for these products violate federal requirements regardless of where they are based.
- Fallback dispensing pathways: Regulatory resilience requires pre-built fallback options. If the primary pharmacy cannot fulfill an order, the program needs an alternate certified pharmacy ready, not a search process that delays the patient's medication by days.
Medication adherence via telehealth depends heavily on the first dispensing experience. Patients who receive their medication late, without instructions, or in a damaged state are significantly less likely to continue the program. That first shipment sets the behavioral expectation for everything that follows.
For programs working within telehealth regulatory compliance frameworks, the practical recommendation is to treat each regulatory requirement as a workflow checkpoint rather than a documentation task. Certification verification, patient agreement execution, and trackable shipping confirmation should all be system-enforced steps, not manual reminders.
Future trends and policy considerations
The regulatory and technological environment shaping the role of medication delivery in telehealth will continue to evolve rapidly through 2026 and beyond. Policymakers and healthcare organizations need to plan for that movement rather than react to it.
Several specific trends deserve attention:
- Ongoing litigation risk: Legal challenges to telehealth prescribing authority for specific drug classes will continue. Programs relying on a single legal pathway for medication delivery are vulnerable. Building multi-pathway compliance models now reduces future disruption.
- Emerging adherence technology: Connected packaging, smart pill dispensers, and automated refill coordination systems are moving from pilot programs into standard practice. These tools provide objective adherence data that clinical teams can act on without requiring patient self-reporting.
- Access equity requirements: Telehealth medication delivery must address the geographic and socioeconomic realities of underserved populations. Platforms that require digital literacy for medication management are not truly accessible. Simplified interfaces, multilingual support, and low-bandwidth compatibility are clinical considerations, not just design preferences.
- Policy alignment with evidence: Policymakers who restrict telehealth medication delivery without engaging the clinical outcome literature risk reducing access for populations that have the most to gain. The evidence on telehealth-supported medication adherence is substantial. Policy frameworks should reflect it.
- Pharmacist integration: The pharmacist's role in telehealth medication management is expanding. Clinical pharmacy services embedded within telehealth platforms, reviewing prescriptions, counseling patients remotely, and managing drug interactions, represent the most underdeveloped high-value function in current telehealth models.
For programs serving rural patients, the benefits of telehealth delivery go well beyond convenience. Telehealth reduces transportation costs, addresses provider shortages, and makes specialist prescribing available in areas where it would otherwise not exist.
My perspective on getting medication delivery right
I've spent considerable time examining how telehealth programs succeed and where they fall apart, and the pattern is consistent. Organizations that treat medication delivery as a logistics problem solve the wrong problem. The clinical team asks: did the patient get better? The logistics team asks: did the package arrive? Both questions matter, but the first one requires the second one plus a great deal more.
What I've found in practice is that the separation between delivery and management is the single most underappreciated design decision in telehealth medication programs. When a care team assumes that delivered medication equals managed medication, adherence suffers, titration lags, and outcomes data looks worse than it should. The pharmacist who follows up three days after a first GLP-1 shipment to confirm the patient understood the injection technique is providing irreplaceable clinical value that no shipping notification can replicate.
The regulatory environment adds a layer that I think many clinical leaders underestimate until it disrupts their program. Legal instability in certain drug categories means that programs without pre-built fallback pathways will face patient harm when their primary dispensing channel is interrupted. Regulatory resilience is not a compliance formality. It is a patient safety requirement.
My strongest recommendation for any program integrating medication delivery into telehealth is this: build your clinical monitoring infrastructure before you scale your delivery volume. The tools exist to do this well. The platforms that use them consistently produce better outcomes and survive regulatory change more effectively.
— Raymond
How Renewmd integrates medication delivery in weight care
For healthcare professionals and policymakers exploring what a well-integrated telehealth medication system looks like in practice, Renewmd offers a concrete model. The platform coordinates provider consultations and medication delivery through licensed U.S. clinicians and pharmacies, with GLP-1 receptor agonists including Semaglutide and Tirzepatide delivered to patients under clinical supervision. Every step from intake to shipment operates within a compliant digital workflow, with no disconnected prescription hand-offs.
Renewmd's approach is particularly relevant for rural and underserved populations where access barriers are highest. The virtual weight management program includes lab testing, ongoing coaching, and medication monitoring within a single care pathway. For professionals designing or evaluating telehealth medication frameworks, Renewmd's model illustrates how delivery logistics and clinical management can function as an integrated system rather than parallel processes.
FAQ
What is the role of medication delivery in telehealth?
Medication delivery in telehealth completes the care episode by getting prescribed treatments to patients, directly affecting adherence, titration support, and clinical outcomes. Without reliable delivery infrastructure, telehealth consultations produce prescriptions that patients may never fill or receive.
How does the Ryan Haight Act affect telehealth prescribing?
The Ryan Haight Act restricts remote prescribing of Schedule II through V controlled substances without a prior in-person evaluation, with specific DEA-registered exceptions. Providers must meet documented compliance criteria before prescribing controlled medications through telehealth channels.
What are REMS requirements for telehealth medication delivery?
REMS programs require pharmacies to hold current certification and ship covered medications using trackable delivery methods. These requirements apply regardless of whether the prescription originated from an in-person or telehealth visit.
How does remote patient monitoring support medication management?
RPM gives care teams real-time data on patient health metrics, enabling proactive medication adjustments and adherence follow-up rather than waiting for scheduled visits. Studies show that higher RPM engagement correlates with significantly better clinical outcomes, including blood pressure control.
What are the main challenges in telehealth medication delivery?
The primary challenges include regulatory instability across drug categories, pharmacy certification verification, patient communication requirements, and the need for fallback dispensing pathways when primary pharmacies cannot fulfill prescriptions. Programs built without these contingencies face care continuity risks when legal or supply conditions shift.