Remote medical supervision is defined as real-time clinical oversight delivered by a licensed physician through live, two-way audiovisual technology rather than physical presence. The industry term for this arrangement is "virtual direct supervision," and it became a permanent feature of U.S. healthcare when the Centers for Medicare and Medicaid Services (CMS) formalized the policy on january 1, 2026. For patients managing chronic conditions through telehealth, this regulatory shift means your care team can legally supervise procedures and services from a distance, without compromising the clinical safety standards that in-person oversight once required.
What is remote medical supervision under the 2026 CMS rules?
Remote medical supervision, formally called virtual direct supervision, requires a supervising physician to be immediately available via video to intervene at any moment during a clinical service. CMS made this definition permanent as of january 1, 2026, replacing the prior requirement that a physician be physically present in the same building. The change applies to most Medicare Part B services, including "incident-to" billing and diagnostic testing.

The policy has clear boundaries. High-risk surgical procedures assigned global surgery indicators 010 or 090 still require onsite physician presence. Virtual supervision does not satisfy those requirements, and attempting to bill them as virtually supervised will result in claim denial. Rural Health Clinics and Federally Qualified Health Centers are also permitted to use virtual supervision under the updated rules.
Technology requirements are specific and non-negotiable:
- Live, two-way audio and video must be active throughout the supervised service
- Phone-only communication does not qualify, regardless of call quality
- The supervising physician must be capable of intervening in real time, not simply reachable by message
- The platform used must support uninterrupted audiovisual connection for the full duration
Pro Tip: Confirm that your telehealth platform explicitly supports "real-time two-way audiovisual" communication before scheduling any supervised service. Platforms that default to audio-only as a fallback can create compliance gaps that trigger Medicare audits.
What is the difference between remote medical supervision and remote patient monitoring?
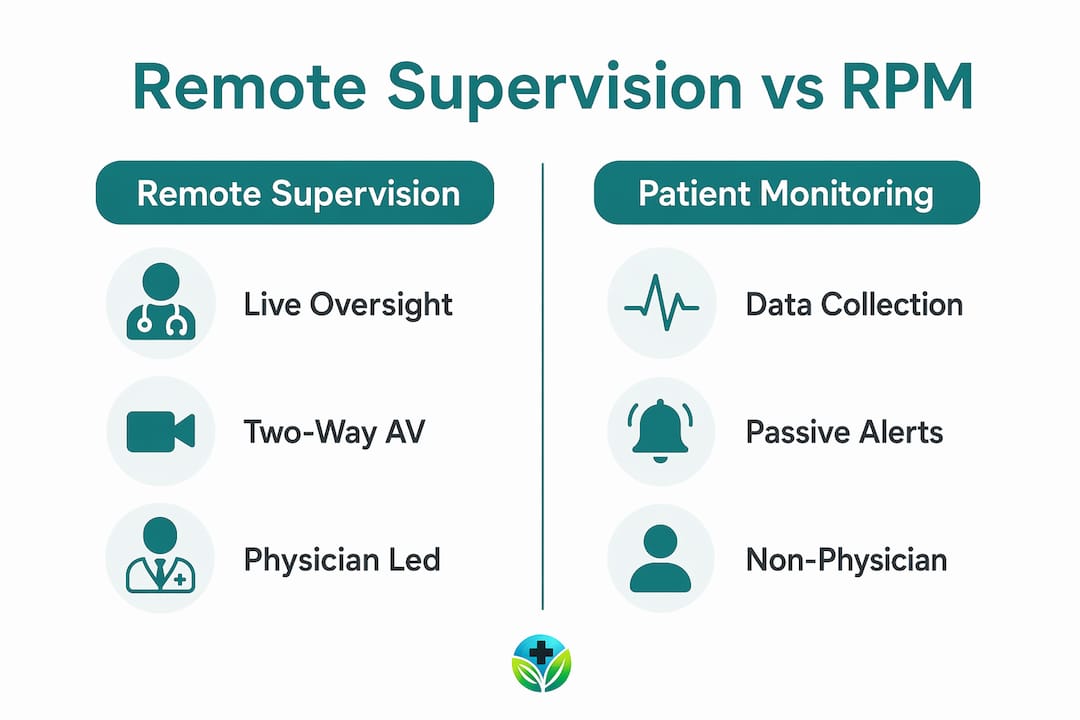
Remote medical supervision and remote patient monitoring (RPM) are related but distinct services. Confusing the two is one of the most common errors patients and providers make when structuring telehealth care.
Remote patient monitoring is defined as the collection and transmission of physiologic data from a patient's home to a provider using internet-connected medical devices. Examples include blood pressure cuffs, continuous glucose monitors, and pulse oximeters that send readings directly to a clinical dashboard. RPM requires at least 16 days of data within a 30-day period to meet billing thresholds, and it includes patient education on device use as a required component.
Remote medical supervision, by contrast, is the live oversight structure under which a physician monitors and directs clinical services in real time. RPM data feeds into that supervisory relationship, but RPM itself is a data collection tool, not a supervision model. Think of RPM as the instrument and virtual direct supervision as the clinician interpreting and acting on what the instrument reports.
The table below clarifies the key differences:
| Feature | Remote medical supervision | Remote patient monitoring |
|---|---|---|
| Core function | Real-time physician oversight of clinical services | Collection and transmission of physiologic data |
| Technology required | Live two-way audio and video | Connected medical devices (e.g., glucose monitors) |
| Physician involvement | Active, immediate availability required | Periodic review of transmitted data |
| CMS billing codes | Incident-to and diagnostic test codes | CPT codes 99453, 99454, 99457 |
| Data frequency requirement | Continuous during supervised service | Minimum 16 days of data per 30-day period |
| Applies to surgery? | No, for high-risk procedures | Not applicable |
RPM and virtual direct supervision often work together. A patient with Type 2 diabetes may use a connected glucometer at home (RPM), while a licensed clinician reviews that data and supervises any follow-up care adjustments through a live video session (virtual direct supervision). Understanding how remote healthcare works as an integrated system helps patients make better decisions about their care setup.
What technology and documentation protocols make virtual supervision compliant?
Compliant virtual direct supervision depends on two equally important pillars: the right technology and thorough documentation. Neither alone is sufficient to withstand a Medicare audit.
On the technology side, the supervising physician must maintain an active, uninterrupted two-way audiovisual connection for the entire duration of the supervised service. Phone-only communication is explicitly excluded as insufficient. The platform must support real-time interaction, not asynchronous messaging or store-and-forward video. Platforms like Zoom for Healthcare, Doxy.me, and similar HIPAA-compliant tools meet the technical standard when configured correctly.
Documentation requirements are equally specific. Audit-ready records must include:
- The name of the telehealth platform used
- Timestamps showing when the supervision session began and ended
- Confirmation that two-way audiovisual connection was active throughout
- The supervising physician's attestation of immediate availability
Generic notes stating that a physician "was available" do not satisfy these requirements. CMS auditors look for explicit, timestamped evidence. Vague documentation is the single most common reason compliant supervision arrangements still result in claim denials.
Pro Tip: Build a documentation template directly into your electronic health record (EHR) system that auto-populates the platform name and prompts for timestamps at session start and close. This removes the risk of incomplete entries during busy clinical days.
The role of licensed clinicians in telemedicine extends beyond clinical judgment. Credentialing compliance across state medical boards and payer contracts adds another layer. Holding multiple state licenses alone does not guarantee compliance. Each payer and state board may impose additional requirements on remote oversight arrangements.
What are the benefits, applications, and limitations of remote medical supervision?
Virtual direct supervision delivers measurable advantages for patients and providers alike, but it also has firm boundaries that patients should understand before relying on it for all care needs.
Benefits for patients and providers:
- Expanded access to care. Patients in rural and underserved areas gain access to specialist oversight without traveling to urban medical centers. Virtual supervision models help address provider shortages in these regions while reducing operational costs significantly.
- Operational efficiency. The Veterans Affairs health system saw telehealth adoption rise from 13% in 2018 to 40% in 2024, with virtual supervision contributing to up to 25% more exams completed and cost reductions of up to 70% in certain programs. That scale of efficiency is not achievable with purely in-person models.
- Flexibility for chronic disease management. Patients managing conditions like hypertension, diabetes, or obesity benefit from continuous oversight without repeated clinic visits. Telehealth-based chronic disease management reduces care gaps that typically occur between appointments.
- Medical training support. Supervising physicians can oversee supervised practitioners across multiple locations simultaneously, expanding training capacity without requiring physical co-location.
- Patient engagement at home. Successful remote supervision depends heavily on patient confidence with home monitoring devices. When patients understand how to use their devices correctly, proactive chronic disease management becomes realistic rather than aspirational.
Limitations to understand:
- High-risk surgery exclusions. Procedures with global surgery indicators 010 or 090 legally require onsite physician presence. Virtual supervision cannot substitute for physical oversight in these cases, and attempting to do so creates both clinical and legal risk.
- Licensing and credentialing complexity. Providers supervising patients across state lines must navigate multiple state medical boards and individual payer contracts. The credentialing burden is real and requires dedicated administrative support.
- Technology access barriers. Patients without reliable broadband or appropriate devices cannot participate in virtual supervision arrangements. This gap disproportionately affects the rural populations the model is designed to serve.
- Patient engagement dependency. Remote supervision is only as effective as the patient's participation. Incomplete device data uploads or missed video sessions break the supervisory chain and create gaps in care.
For patients considering telepharmacy as part of their remote care plan, understanding medication management at a distance is a practical complement to virtual supervision.
Key Takeaways
Remote medical supervision is a legally defined, technology-dependent oversight model that requires live two-way audiovisual connection, explicit documentation, and physician immediate availability to satisfy CMS compliance standards.
| Point | Details |
|---|---|
| Virtual supervision is now permanent | CMS made virtual direct supervision a permanent Medicare policy as of january 1, 2026. |
| Surgery exclusions apply | High-risk procedures with global indicators 010 or 090 still require onsite physician presence. |
| RPM and supervision are distinct | RPM collects physiologic data; virtual supervision is the live clinical oversight structure that uses that data. |
| Documentation must be explicit | Records must include platform name, timestamps, and audiovisual confirmation to survive audits. |
| Patient engagement drives outcomes | Remote supervision works best when patients actively use monitoring devices and attend video sessions consistently. |
Why the shift to virtual supervision matters more than most patients realize
The 2026 CMS rule change is not just a billing update. It represents a fundamental rethinking of what "presence" means in clinical medicine. For years, the assumption was that a physician had to be physically nearby to maintain meaningful oversight. That assumption was largely a product of technological limitation, not clinical necessity.
What I find most significant is that virtual direct supervision retains full supervisory responsibility. The physician is not simply "on call" in a loose sense. The standard requires immediate availability for intervention, which means the clinical accountability is identical to in-person supervision. The only thing that changed is the medium.
The practical challenge is uptake. Many practices have the technology but lack the documentation discipline to use it compliantly. A single missing timestamp or a vague attestation note can undo an otherwise compliant supervision arrangement during an audit. The gap between having the right tools and using them correctly is where most compliance failures occur.
The future of this model depends on two things: better technology integration within EHR systems to automate documentation, and patient education that builds genuine confidence with home monitoring devices. A remote patient support checklist is a practical starting point for patients and caregivers who want to get that foundation right. The clinical potential of virtual supervision is real. Realizing it consistently requires the same rigor applied to in-person care.
— Raymond
Renewmd and medically supervised telehealth care
Renewmd is a telemedicine platform built around the principle that medically supervised care should be accessible, transparent, and clinically grounded. For patients managing weight-related conditions, Renewmd provides integrated programs that include licensed U.S. clinician consultations, GLP-1 medications like Semaglutide and Tirzepatide, lab testing, and ongoing coaching, all delivered through a fully digital process. Every treatment plan operates under professional oversight, with no hidden fees and no gaps between clinical guidance and medication delivery. Patients who want to understand how telehealth and virtual weight care work in practice will find Renewmd's model a clear example of remote supervision applied to chronic disease management. To connect with a licensed provider and begin a supervised weight management consultation, visit Renewmd's start page.
FAQ
What is remote medical supervision in simple terms?
Remote medical supervision is when a licensed physician oversees a clinical service through live video and audio rather than being physically present. CMS permanently recognized this as equivalent to in-person direct supervision as of january 1, 2026.
Does virtual supervision apply to all medical procedures?
No. Virtual direct supervision applies to most Medicare Part B services, but high-risk surgical procedures with global surgery indicators 010 or 090 still require onsite physician presence.
How is remote patient monitoring different from virtual supervision?
Remote patient monitoring collects physiologic data from connected devices at home, while virtual direct supervision is the live physician oversight structure used to act on that data in real time.
What documentation is required for virtual direct supervision?
Records must include the telehealth platform name, session timestamps, duration of supervision, and explicit confirmation that two-way audiovisual connection was active throughout the service.
Can patients in rural areas benefit from remote medical supervision?
Yes. Virtual supervision is specifically designed to expand care access in rural and underserved areas, and research from the Veterans Affairs system shows significant efficiency gains from telehealth models that include virtual oversight.