Pharmacological weight management is the medical use of prescription medications to help individuals lose weight and manage obesity-related health conditions by targeting the biological mechanisms that drive excess weight gain. Clinically, this approach is called pharmacotherapy for obesity, and it has undergone a significant transformation with the arrival of GLP-1 receptor agonists like semaglutide and dual GLP-1/GIP receptor agonists like tirzepatide. These agents produce weight loss up to 20% of total body weight, a result that rivals bariatric surgery without the invasiveness. For anyone evaluating medications for weight management, understanding how these drugs work, who qualifies, and what realistic outcomes look like is the foundation of an informed decision.
What is pharmacological weight management and how do medications work?
Weight management medications work through several distinct biological pathways, and the mechanism determines both the drug's efficacy and its side effect profile. GLP-1 receptor agonists like semaglutide mimic the glucagon-like peptide-1 hormone, which signals satiety to the brain via the hypothalamus, slows gastric emptying, and reduces appetite. The result is a lower caloric intake without requiring willpower alone to sustain it.
Tirzepatide goes further by activating both GLP-1 and GIP receptors simultaneously. GIP, or glucose-dependent insulinotropic polypeptide, enhances insulin secretion and directly influences fat tissue metabolism. This dual incretin receptor agonism produces greater metabolic effects than GLP-1 activation alone, which explains why tirzepatide consistently outperforms earlier agents in clinical trials.

Orlistat operates through a completely different mechanism. It inhibits pancreatic lipase, the enzyme responsible for breaking down dietary fat in the gut, so roughly 30% of consumed fat passes through unabsorbed. This reduces caloric intake from fat but does not affect appetite or hormonal signaling.
Oral agents like naltrexone-bupropion target the central nervous system. Bupropion activates pro-opiomelanocortin neurons in the hypothalamus, while naltrexone blocks the feedback loop that would normally suppress those neurons, sustaining the appetite-reducing signal. Phentermine-topiramate combines a sympathomimetic stimulant with an anticonvulsant to reduce appetite and increase satiety through separate pathways.
- GLP-1 receptor agonists (semaglutide, liraglutide): reduce appetite, slow gastric emptying, improve glycemic control
- Dual GLP-1/GIP agonists (tirzepatide): enhanced metabolic and appetite effects via two receptor pathways
- Lipase inhibitors (orlistat): block dietary fat absorption in the gut
- CNS agents (naltrexone-bupropion, phentermine-topiramate): modulate hunger and reward pathways in the brain
Pro Tip: If you experience nausea on a GLP-1 agonist, it typically peaks in the first four to eight weeks and decreases significantly as your body adjusts to the medication. Eating smaller, lower-fat meals during this period helps considerably.
How do FDA-approved weight loss drugs compare?
Six medications currently hold FDA approval for chronic weight management in adults, and they differ substantially in efficacy, administration route, and the patient populations they suit best.
| Medication | Average weight loss | Administration | Common side effects | Approved population |
|---|---|---|---|---|
| Tirzepatide | 15.0%–20.9% | Weekly injection | Nausea, diarrhea | Adults, adolescents 12+ |
| Semaglutide | 10.9%–14.9% | Weekly injection or daily oral | Nausea, vomiting | Adults, adolescents 12+ |
| Liraglutide | ~5%–8% | Daily injection | Nausea, injection site reactions | Adults, adolescents 12+ |
| Orlistat | ~3%–5% | Three times daily oral | Oily stools, GI discomfort | Adults, adolescents 12+ |
| Naltrexone-bupropion | ~5%–9% | Twice daily oral | Headache, nausea, elevated BP | Adults |
| Phentermine-topiramate | ~7%–11% | Daily oral | Increased heart rate, dry mouth | Adults |
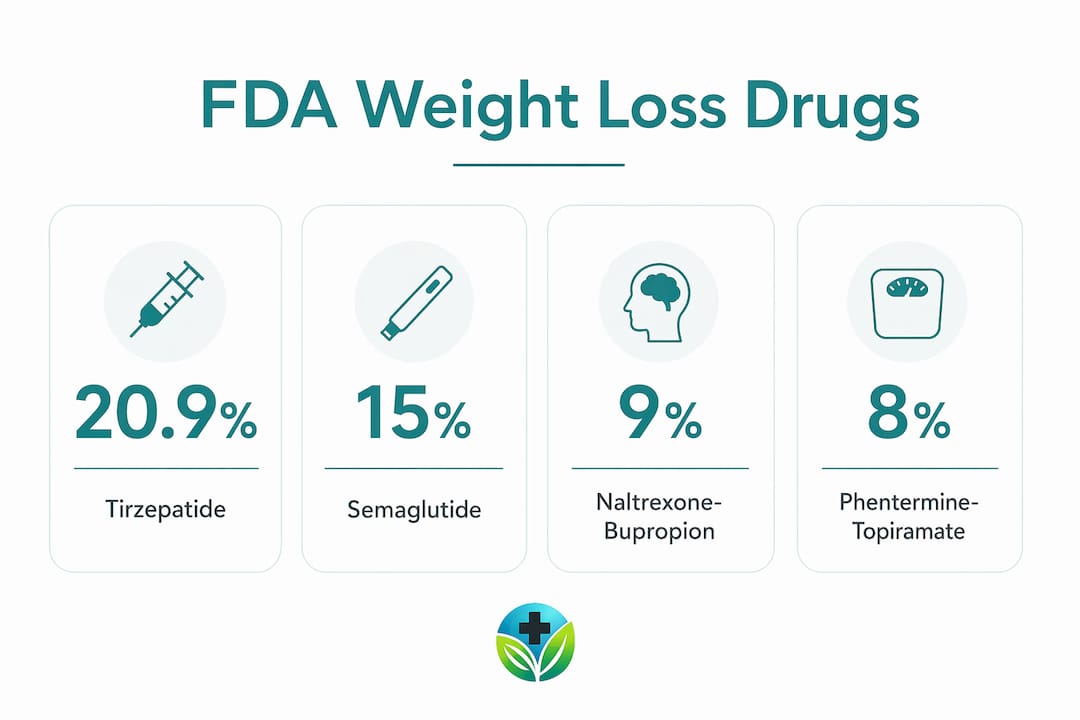
Tirzepatide's clinical trial results are the most striking in this class. At doses of 5 mg, 10 mg, and 15 mg, participants achieved weight reductions of 15.0%, 19.5%, and 20.9% respectively. That level of pharmacological weight loss was not achievable with any prior non-surgical intervention, which is why prescribing patterns have shifted sharply toward this agent.
Semaglutide, marketed as Wegovy for weight management and Ozempic for type 2 diabetes, produces 10.9%–14.9% weight loss and also carries FDA approval for reducing major adverse cardiovascular events in adults with established cardiovascular disease. The GLP-1 efficacy comparison between these newer agents and older oral therapies shows a clear performance gap that is difficult to ignore.
Oral options remain clinically relevant. Naltrexone-bupropion and phentermine-topiramate suit patients who prefer pills, cannot tolerate injections, or have specific contraindications to GLP-1 agonists. Orlistat is available over the counter at a lower dose and carries no cardiovascular or CNS effects, making it an option for patients with complex medication interactions.
Pro Tip: Ask your provider about the oral formulation of semaglutide (Rybelsus) if you are interested in GLP-1 therapy but prefer to avoid injections. It requires specific dosing conditions, including taking it on an empty stomach with a small amount of water, but it delivers meaningful weight loss results.
Who qualifies for weight management medication?
FDA eligibility criteria for weight management medications are defined by BMI thresholds and the presence of obesity-related health conditions. Providers prescribe these medications for adults with a BMI of 30 or higher, or for adults with a BMI of 27 or higher who have at least one weight-related comorbidity such as type 2 diabetes, hypertension, dyslipidemia, or obstructive sleep apnea.
Several medications, including tirzepatide, semaglutide, liraglutide, orlistat, and phentermine-topiramate, now carry FDA approval for adolescents aged 12 and older, reflecting growing recognition that obesity in younger populations requires medical intervention, not just behavioral counseling.
The initial patient evaluation is thorough by design. Providers review complete medical history, conduct a physical examination, and order laboratory tests to rule out secondary causes of weight gain such as hypothyroidism or Cushing's syndrome, and to identify contraindications. This process is not bureaucratic. It directly shapes which medication is selected.
Personalization goes beyond BMI. A patient with type 2 diabetes and cardiovascular risk factors is a strong candidate for tirzepatide or semaglutide because both drugs address all three conditions simultaneously. A patient with a history of eating disorders or mood disorders may be better suited to a different agent. The EASO treatment algorithm for obesity pharmacotherapy explicitly accounts for comorbidities like sleep apnea and cardiovascular risk when guiding drug selection, moving well beyond simple weight loss percentages as the deciding factor.
- BMI ≥30 with no comorbidities
- BMI ≥27 with at least one comorbidity (type 2 diabetes, hypertension, dyslipidemia, sleep apnea)
- Adolescents aged 12 and older for select medications
- No secondary cause of obesity identified through lab evaluation
- No contraindications specific to the chosen agent
What are the benefits and limitations of pharmacological weight management?
The clinical benefits of effective weight loss drugs extend well beyond the number on a scale. Tirzepatide and semaglutide both demonstrate cardiovascular and metabolic improvements including reduced risk of major adverse cardiovascular events, improved glycemic control, and in some patients, remission of type 2 diabetes. These outcomes matter because obesity-related complications, not obesity itself, are the primary drivers of reduced life expectancy.
Weight loss achieved through pharmacotherapy also exceeds what lifestyle modification alone typically produces. Most structured diet and exercise programs yield 3%–5% sustained weight loss over 12 months. The newer GLP-1 and dual agonist agents produce three to five times that result, which crosses the clinical threshold where meaningful reductions in blood pressure, liver fat, and joint load become measurable.
"Pharmacotherapy has transformed obesity care, offering weight loss results comparable to bariatric surgery with less invasiveness, with new agents achieving average weight loss of 15%–25%." StatPearls, NCBI Bookshelf
The limitations are real and worth understanding clearly. Side effects, primarily nausea, vomiting, and diarrhea with GLP-1 agonists, cause some patients to reduce doses or discontinue treatment. Cost remains a significant barrier. Branded GLP-1 medications can exceed $1,000 per month without insurance coverage, and coverage varies widely by plan and indication.
The most clinically important limitation is the chronic nature of this treatment. Weight regain after stopping medication is well documented, often recovering two-thirds of lost weight within a year of discontinuation. This is not a failure of the drug. It reflects the biology of obesity as a chronic, relapsing condition that requires sustained management, much like hypertension or type 2 diabetes.
How to integrate medication into a sustainable weight loss plan
Medication works most effectively when it is one component of a broader treatment strategy, not the entire plan. The EASO guidelines advocate integrating pharmacotherapy with lifestyle modifications including nutrition counseling, physical activity, and behavioral therapy for long-term management of obesity.
Follow these steps to build a plan that supports lasting results:
- Set realistic, health-focused goals. Target a 5%–10% reduction in body weight over the first six months. This range produces measurable improvements in blood pressure, blood sugar, and cholesterol before you reach an ideal weight.
- Establish a nutrition baseline. Work with a registered dietitian to identify eating patterns that complement your medication. GLP-1 agonists reduce appetite significantly, so protein and micronutrient density in smaller meals becomes more important.
- Add structured physical activity gradually. Start with 150 minutes of moderate activity per week, as recommended by the American College of Sports Medicine. Resistance training preserves lean muscle mass during rapid weight loss, which protects metabolic rate.
- Monitor progress and side effects consistently. Schedule follow-up appointments at 4 weeks, 12 weeks, and 6 months to assess weight, labs, and tolerability. Dose adjustments are common and expected.
- Use digital tools to support adherence. Apps that track food intake, medication timing, and physical activity improve long-term adherence. Digital tools for weight care provide continuous support between clinical visits, which is where most adherence challenges occur.
Pro Tip: Patients who combine pharmacotherapy with behavioral counseling maintain significantly more weight loss at 12 months than those using medication alone. Even monthly check-ins with a health coach make a measurable difference in outcomes.
Behavioral therapy addresses the psychological dimensions of eating, including emotional eating, food environment management, and stress responses. These factors do not disappear when appetite decreases. Addressing them directly reduces the risk of weight regain if medication is eventually tapered or stopped.
Key takeaways
Pharmacological weight management produces clinically significant, sustained weight loss when FDA-approved medications are combined with personalized lifestyle modification and long-term medical supervision.
| Point | Details |
|---|---|
| Tirzepatide leads in efficacy | Clinical trials show up to 20.9% total body weight loss, the highest of any approved agent. |
| Eligibility requires BMI thresholds | Adults with BMI ≥30, or ≥27 with a comorbidity, qualify for prescription weight management medications. |
| Medication alone is not sufficient | Long-term success requires combining pharmacotherapy with nutrition, activity, and behavioral support. |
| Stopping medication risks regain | Obesity is a chronic condition; discontinuing medication without a maintenance plan typically leads to weight returning. |
| Personalization drives outcomes | Drug selection should account for comorbidities, metabolic profile, and patient preference, not BMI alone. |
Why I think we are finally treating obesity the right way
For years, the clinical conversation around obesity defaulted to "eat less, move more," as if the biology of hunger and fat storage were simply a matter of discipline. What the GLP-1 and dual agonist era has done is make the underlying biology undeniable. When patients lose 15%–20% of their body weight on tirzepatide and their blood pressure normalizes, their sleep apnea resolves, and their type 2 diabetes goes into remission, it becomes impossible to argue that obesity was a lifestyle choice rather than a disease.
What I find most significant is not the weight loss numbers themselves. It is the shift in how providers and patients are beginning to think about treatment duration. The parallel to hypertension management is exact. No one expects a patient to take a blood pressure medication for six months and then stop. The same logic applies here, and the EASO chronic disease framework for obesity is finally codifying that expectation.
The patients who do best are those who understand from the start that medication is one tool within a broader strategy. Combining it with metabolic health optimization and behavioral support produces outcomes that neither approach achieves alone. The future of this field will bring more targeted agents and better personalization. But the foundational principle, treating obesity as a chronic, biology-driven disease requiring sustained multi-modal care, is already established. The tools are here. The evidence is clear. The question now is whether patients and providers will use them with the long-term commitment the condition requires.
— Raymond
Start your weight management plan with Renewmd
Renewmd offers fully supervised pharmacological weight management programs built around FDA-approved medications including Semaglutide and Tirzepatide, delivered entirely through telemedicine. Every program includes a licensed provider consultation, lab testing, medication delivery from U.S. pharmacies, and ongoing coaching, with no hidden fees. If you are ready to move from understanding your options to acting on them, begin your GLP-1 journey with a clinical intake process designed to match you with the right medication and support structure. Renewmd also provides digital adherence tools to help you stay on track between visits, because consistent support between appointments is where long-term results are built.
FAQ
What is pharmacological weight management?
Pharmacological weight management is the use of prescription medications to reduce body weight by targeting biological mechanisms such as appetite regulation, fat absorption, and metabolic signaling. It is also called pharmacotherapy for obesity and is prescribed alongside lifestyle modification for adults who meet BMI eligibility criteria.
How does weight management medication work?
GLP-1 receptor agonists like semaglutide signal satiety to the brain and slow gastric emptying, while dual agonists like tirzepatide also activate GIP receptors to enhance metabolic effects. Other agents like orlistat block fat absorption in the gut, and CNS-acting drugs like naltrexone-bupropion reduce appetite through brain reward pathways.
What are the most effective weight loss drugs available?
Tirzepatide produces the highest documented weight loss of any approved agent, with clinical trial results of up to 20.9% total body weight loss. Semaglutide follows closely, achieving 10.9%–14.9% weight loss in trials, and both carry additional cardiovascular and metabolic benefits.
Who is eligible for prescription weight loss medications?
Adults with a BMI of 30 or higher, or a BMI of 27 or higher with at least one weight-related comorbidity such as type 2 diabetes or hypertension, qualify for FDA-approved weight medications. Several medications are also approved for adolescents aged 12 and older.
Will I regain weight if I stop taking the medication?
Weight regain after stopping medication is common because obesity is a chronic, biology-driven condition. Sustained success requires either long-term medication use or a well-structured maintenance plan combining behavioral therapy and lifestyle modification to preserve results.