Weight management is rarely as simple as eating less and moving more. Over 73% of U.S. adults have overweight or obesity, yet most people cycling through diets, exercise programs, and willpower-based strategies see limited lasting results. The reality is that weight regulation involves complex hormonal, metabolic, and behavioral systems that often require clinical support to address effectively. For adults with a BMI of 27 or higher, medically supervised options including GLP-1 receptor agonists, the class of drugs behind medications like Semaglutide and Tirzepatide, have fundamentally changed what is possible through both in-person and telehealth care.
Table of Contents
- What weight management really means
- Medically supervised weight loss: Options and approaches
- GLP-1 therapies: How they work and what to expect
- Risks, side effects, and best practices
- Nuances, emerging therapies, and telehealth's future
- Weight management: Hard truths and fresh perspectives
- Get started with telehealth weight management and GLP-1 care
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Medical supervision matters | Medically supervised weight management is safer and more effective for adults with BMI 27+. |
| GLP-1 therapies boost results | GLP-1 medications show clinically significant weight loss, but require careful monitoring for side effects. |
| Lifestyle remains essential | Diet and activity are foundational—even when using advanced approaches like GLP-1 therapies. |
| Muscle preservation is key | Pair resistance training and protein with GLP-1s to reduce muscle loss and maximize health benefits. |
| Telehealth expands access | Virtual consults and prescriptions make supervised care easier to access for U.S. adults. |
What weight management really means
Weight management is not a single action. It is a sustained process that draws on lifestyle modification, behavioral support, and, for many adults, pharmacological (medication-based) intervention. According to the National Institute of Diabetes and Digestive and Kidney Diseases, weight management involves adopting healthy eating and physical activity habits to safely reduce and maintain weight long term, with medically supervised options including GLP-1 therapies via telehealth recommended when lifestyle alone is insufficient.
Understanding where you fall on the BMI (Body Mass Index) scale helps clarify which interventions are medically appropriate. BMI is not a perfect measure, but it remains the standard clinical tool for assessing weight category and treatment eligibility.
| BMI range | Category | Medical eligibility |
|---|---|---|
| 18.5 to 24.9 | Normal weight | Standard lifestyle guidance |
| 25.0 to 26.9 | Overweight | Lifestyle focus, monitoring |
| 27.0 to 29.9 | Overweight with comorbidities | Eligible for pharmacotherapy |
| 30.0 and above | Obesity | Eligible for full medical program |
Comorbidities, meaning related health conditions such as hypertension, type 2 diabetes, or sleep apnea, lower the BMI threshold for medication eligibility to 27. That distinction matters. It means millions of adults who may not think of themselves as candidates for medical weight care actually qualify.
Why does supervised care produce better outcomes than solo efforts? The answer lies in accountability, clinical monitoring, and access to interventions that are simply unavailable over the counter. Reviewing effective weight management strategies shows how combining behavioral tools with clinical support consistently outperforms lifestyle-only approaches.
Key reasons supervised care works:
- Clinicians can identify hormonal or metabolic factors driving weight gain
- Regular monitoring prevents nutrient deficiencies and muscle loss
- Behavioral coaching addresses the psychological drivers of eating patterns
- Medication titration (gradual dose adjustment) is safer under clinical oversight
"When lifestyle changes alone are insufficient, medically supervised weight management shifts from optional to medically indicated for adults with BMI 27 or higher with related health conditions." — National Institute of Diabetes and Digestive and Kidney Diseases
Medically supervised weight loss: Options and approaches
Medical weight management programs are built around several integrated components. No single element works in isolation. The strongest outcomes come when diet, physical activity, behavioral support, and medication work together under clinical guidance.
Structured programs typically involve:
- Dietary assessment and planning with personalized calorie and macronutrient targets
- Physical activity prescription targeting at least 150 minutes of moderate activity per week
- Behavioral support including counseling for emotional eating and habit formation
- Pharmacotherapy using FDA-approved medications when clinically appropriate
- Ongoing monitoring of labs, weight, blood pressure, and metabolic markers
Telehealth has significantly expanded who can access this level of care. Telehealth programs now offer virtual consultations, prescription management, remote monitoring, and regular check-ins that mirror the quality of in-person care. Programs such as Amazon One Medical's GLP-1 program illustrate how virtual weight management platforms can provide structured protocols, prescriptions, and monitoring through digital channels, making care accessible for adults who live far from specialized clinics or have limited time.

| Approach | Lifestyle only | Medically supervised telehealth |
|---|---|---|
| Personalized plan | General guidance | Clinician-tailored |
| Medication access | None | Prescription via licensed provider |
| Monitoring | Self-directed | Lab tests, provider check-ins |
| Behavioral support | Self-help resources | Integrated coaching |
| Average weight loss | 3 to 5% | 10 to 22% depending on medication |
The numbers in that last row are not trivial. A 10 to 22% reduction in body weight for someone weighing 250 pounds means 25 to 55 pounds. That scale of change has measurable effects on blood pressure, blood sugar, joint health, and cardiovascular risk.
Pro Tip: If you have been told your BMI is in the 27 to 29.9 range and you also have high blood pressure or prediabetes, ask your provider specifically about GLP-1 eligibility. Many adults in this range qualify for medication but are never offered it.
GLP-1 therapies: How they work and what to expect
GLP-1 receptor agonists, abbreviated from glucagon-like peptide-1 receptor agonists, represent the most significant pharmacological advance in weight management in decades. These medications mimic a hormone your gut naturally releases after eating, signaling your brain that you are full while also slowing gastric emptying and improving insulin response.
The FDA has approved several GLP-1 medications for weight management. Semaglutide (Wegovy) and Tirzepatide (Zepbound)00059-2/fulltext) are approved for adults with BMI 30 or higher, or BMI 27 or higher with at least one weight-related condition. Tirzepatide works on two receptors (GLP-1 and GIP), giving it a dual-agonist mechanism that contributes to its stronger effect profile.
The mechanism is worth understanding because it explains why these medications work when others have not:
- Central appetite suppression: GLP-1 acts on the hypothalamus, the brain region that regulates hunger and satiety, reducing appetite without requiring conscious restriction
- Delayed gastric emptying: Food moves more slowly through the stomach, extending feelings of fullness after meals
- Improved insulin secretion: The pancreas releases insulin more effectively in response to blood sugar, benefiting people with insulin resistance
- Reduced glucagon: Lower glucagon levels prevent excessive glucose release from the liver
- Improved lipid and inflammation markers: Secondary benefits that reduce cardiovascular risk over time
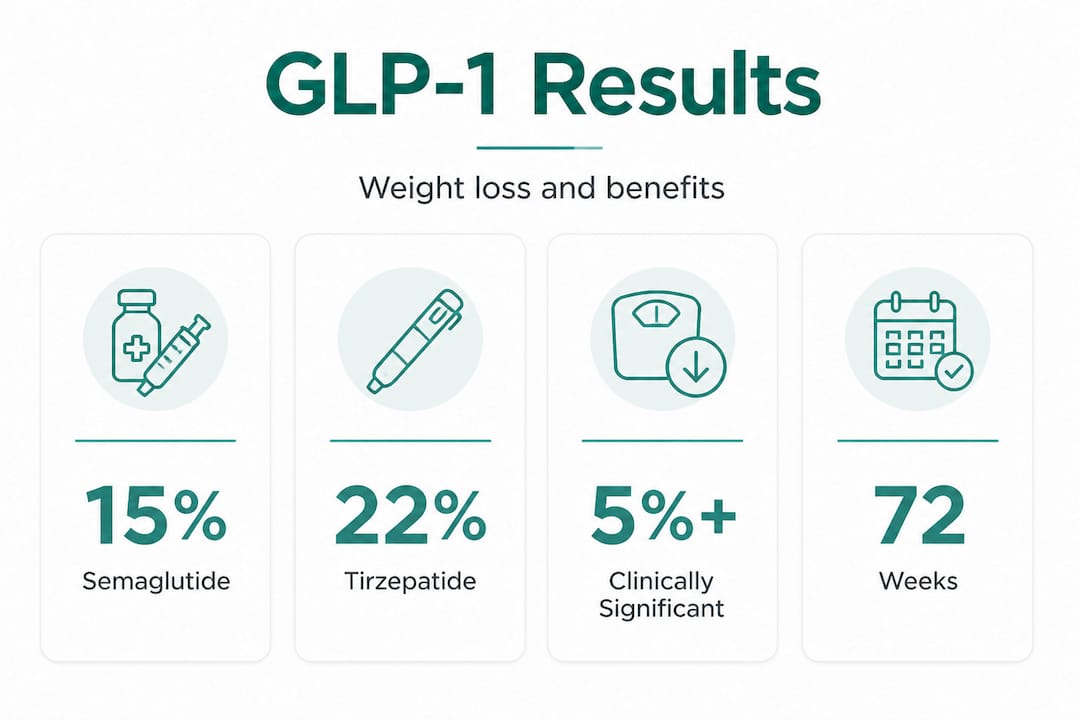
| Medication | Mechanism | Average weight loss at 72 weeks |
|---|---|---|
| Semaglutide (Wegovy) | GLP-1 agonist | ~15% body weight |
| Tirzepatide (Zepbound) | GLP-1 and GIP dual agonist | ~20 to 22% body weight |
| Older medications | Various | 3 to 8% body weight |
Clinicians generally consider a weight loss of 5% or more clinically significant because that threshold produces meaningful reductions in blood pressure, blood sugar, and cardiovascular risk. A 5 to 10% reduction in body weight lowers blood pressure by approximately 5 to 10 mmHg, which translates to measurable protection against stroke and heart disease.
For people managing GLP-1 for hypothalamic obesity, where the brain's weight regulation centers are affected, these central mechanisms are especially relevant. Similarly, GLP-1 for active people requires thoughtful dosing to preserve performance while achieving metabolic goals.
Risks, side effects, and best practices
Successful weight loss is about more than the number on the scale. Maintaining muscle, managing side effects, and knowing who should not use these medications are all part of responsible treatment.
The most commonly reported side effects with GLP-1 therapies include:
- Nausea: Reported by up to 72% of patients, usually most intense during dose escalation and typically resolving within a few weeks
- Vomiting and diarrhea: Less common but related to gastric effects; manageable with slower titration
- Constipation: Particularly noted with Tirzepatide
- Fatigue: Often temporary, related to reduced caloric intake during early weeks
- Muscle loss: A significant concern, especially in older adults or those losing weight rapidly
Muscle loss is worth a focused discussion. When your body loses weight rapidly, it does not always distinguish between fat and lean tissue. GLP-1 and muscle loss can become a serious concern when patients do not actively protect muscle through resistance training and adequate protein intake.
Clinical guidance recommends resistance training two to three times per week and a protein intake of 1.2 to 1.5 grams per kilogram of body weight per day to mitigate this risk. Strategies for avoiding muscle loss on GLP-1s should be part of any supervised program, and strength training with GLP-1 is not only safe but actively recommended.
Contraindications (conditions that rule out use) include:
- Personal or family history of medullary thyroid carcinoma (a specific thyroid cancer type)
- Multiple endocrine neoplasia syndrome type 2 (MEN2)
- History of pancreatitis in some cases
- Pregnancy or planned pregnancy
"GLP-1 therapy requires ongoing monitoring for GI tolerance, renal function, and thyroid risk markers. Medical supervision is not optional. It is how safe outcomes are achieved." — Clinical guidance summary, Risks and Mitigation for GLP-1 Therapy
Pro Tip: If you experience persistent nausea beyond four to six weeks at a given dose, speak with your provider before pushing to the next dose tier. Slower titration dramatically improves tolerability without reducing long-term outcomes.
Nuances, emerging therapies, and telehealth's future
The landscape of weight management pharmacotherapy is evolving rapidly. GLP-1 dual agonists like Tirzepatide already outperform single-agonist Semaglutide in trials. Now, triple agonists that target GLP-1, GIP, and glucagon receptors simultaneously are showing weight loss results approaching 24% in clinical trials, which would represent a new ceiling for pharmacological efficacy.
Several key distinctions are shaping current clinical thinking:
| Approach | Weight loss potential | Supervision level needed |
|---|---|---|
| Lifestyle only | 3 to 5% | Low to moderate |
| GLP-1 single agonist | 12 to 16% | High, requires clinical monitoring |
| GLP-1/GIP dual agonist | 18 to 22% | High, with regular labs and check-ins |
| Triple agonist (emerging) | Up to 24% | Clinical trial level at present |
Telehealth's role is growing alongside this drug pipeline. Platforms that offer modern GLP-1 care are increasingly integrating mental health support, nutrition coaching, and lab monitoring into a single digital experience. However, one important nuance is that telehealth should complement, not replace, your relationship with a primary care provider. Integrated care, where your telehealth weight management team communicates with your broader medical team, leads to safer outcomes.
It is also worth naming the misconception that GLP-1 medications offer a permanent cure. They do not. These are highly effective tools that work best as part of a long-term management plan. Weight regain following discontinuation is well-documented, which underscores why these medications are best framed as chronic disease management rather than short-term intervention.
Important realities to keep in mind:
- GLP-1 therapies are superior to prior weight loss medications but require sustained use for sustained results
- Telehealth expands access significantly, particularly for underserved populations and those in rural areas
- Emerging multi-agonist drugs will likely offer greater efficacy but may also carry new risk profiles requiring updated monitoring protocols
- Long-term integration of behavioral, nutritional, and pharmacological support remains the gold standard
Weight management: Hard truths and fresh perspectives
Most mainstream guides present weight management as a problem with a solution. Eat better. Move more. Take this medication. But the honest picture is more complicated, and people seeking care deserve to hear it.
Obesity is now recognized as a chronic disease requiring lifelong management, not a temporary condition to be solved and set aside. GLP-1 therapies are not magic, despite how they are sometimes portrayed. They are highly effective pharmacological tools that produce outcomes lifestyle changes alone rarely achieve. But they work best when paired with behavioral change, nutritional support, and clinical oversight.
Here is what most articles skip over: the people who see the best results with GLP-1 therapies are not the ones who simply take the medication and wait. They are the ones who use the reduced appetite as an opportunity to build better habits, who prioritize protein and resistance training to protect muscle, and who maintain an ongoing relationship with a clinical team. The medication creates a window. What you do in that window determines how durable your results are.
There is also a quiet risk in framing GLP-1s as purely metabolic tools. Weight management involves psychology, social context, and lifestyle patterns that no medication addresses on its own. Programs that acknowledge this, and build behavioral support into the treatment model, consistently outperform those that treat medication as a standalone solution.
The future belongs to integrated care, where telehealth platforms, licensed clinicians, nutritional guidance, and FDA-approved pharmacotherapy work together under one transparent, medically sound structure. Exploring medically supervised weight care strategies reveals how this integration looks in practice and why it matters for long-term success.
Get started with telehealth weight management and GLP-1 care
If you are an adult with a BMI of 27 or higher and you are ready to move beyond guesswork, RenewMD.clinic offers fully integrated telehealth weight management programs built around Semaglutide and Tirzepatide. Starting with understanding what GLP-1s do provides a solid clinical foundation before beginning treatment. From there, weight management digital tools help you track progress and stay accountable between provider check-ins. For those weighing their options, a clear GLP-1 efficacy comparison breaks down how Semaglutide and Tirzepatide perform against each other and older treatments. RenewMD.clinic's programs include provider consultations, lab testing, medication delivery, and coaching, all with transparent pricing and no hidden fees, delivered entirely through licensed U.S. clinicians and pharmacies.
Frequently asked questions
Who is eligible for medically supervised weight management with GLP-1 therapies?
Adults with a BMI of 30 or higher, or a BMI of 27 or higher with at least one weight-related condition such as hypertension or type 2 diabetes, qualify for GLP-1 therapy00059-2/fulltext) under medical supervision.
How much weight loss can I expect from GLP-1 medications?
Most patients achieve roughly 15 to 22% body weight reduction over 72 weeks, with Tirzepatide outperforming Semaglutide in head-to-head comparisons; actual results depend on medication, adherence, and clinical support.
What are common side effects with GLP-1 therapies?
Nausea is the most frequently reported side effect, affecting up to 72% of patients, though it is usually transient; muscle loss is also a risk, best managed with resistance training and adequate protein intake.
Is telehealth as effective as in-person care for weight management?
Telehealth programs provide the same core services as traditional in-person care, including consultations, prescriptions, and monitoring, expanding access without compromising the quality of clinical supervision.
Will I regain weight after stopping GLP-1 treatment?
Weight regain is common after discontinuing GLP-1 therapy, which is why these medications are best approached as part of a long-term management plan rather than a short-term course of treatment.